Treatment

Treatment
Medication, splint or surgery?
Carpal tunnel syndrome (CTS) can be treated conservatively when it first presents – this means it can be cured without the need for surgery. However, advanced CTS is less reversable – at most, using conservative treatment, you can only alleviate the symptoms. Without surgery the symptoms won’t completely disappear. In these cases, only the surgical route can help. There are various types of surgery to choose from. I use the endoscopic variant, which is minimally invasive. Here, a skin incision measuring only 7mm is made. This surgical technique is especially gentle, with a rapid recovery – you can return to work and your everyday life much faster.
TIP
You may find various alternative treatments for carpal tunnel syndrome on the internet. These range from vitamin supplements to special equipment and exercises. There’s little to no evidence of their effectiveness, which is why they aren’t mentioned here.

FOR MILD COMPLAINTS OR THE BEGINNINGS OF CARPAL TUNNEL SYNDROME (CTS)
Early-stage CTS can be treated effectively with physiotherapy. By doing various exercises, you can improve your symptoms or even make them disappear completely. If your CTS has been caused by specific events, such as heavy manual work, an accident at work, pregnancy, etc., then these conservative treatments can cause it to completely regress. You can also take oral anti-inflammatories to ease your symptoms. Cryotherapy (cold therapy) is another effective method to ease acute pain. Carpal tunnel splints (available from orthopaedic shops) can be worn at night to significantly improve or even eliminate night pain.
- Corticosteroid injections are also an option, though I usually advise my patients against it. The effects are only short-lasting.
- If you’re pregnant, you should always wait – in most cases, the symptoms will go away on their own.
If the symptoms persist for months or even years, the CTS will no longer regress on its own. Rather, the symptoms will increase over time. In this case, surgery is the recommended treatment.

FOR SEVERE OR LONG-LASTING SYMPTOMS: SURGICAL TREATMENT
During a carpal tunnel operation, the transverse ligament (flexor retinaculum), which spans the carpal tunnel, is severed. This creates more room for the nerve (N. nedianus) underneath it. There are many types of surgical techniques, which can be divided into open or minimally invasive procedures.
- Open surgical technique:
This is the traditional surgical technique for CTS. A longitudinal skin incision is made between the ball of the thumb and the ball of the little finger. The incision is usually 50-60 mm long, located in the hand’s stress zone. The flexor retinaculum, which spans the carpal tunnel, is then visible and can be carefully split.
- Minimally invasive surgical technique:
This differs from the open technique only in the length of the incision. The skin incision measures 10-20 mm and is also located in the hand’s stress zone.
- Endoscopic surgical technique:
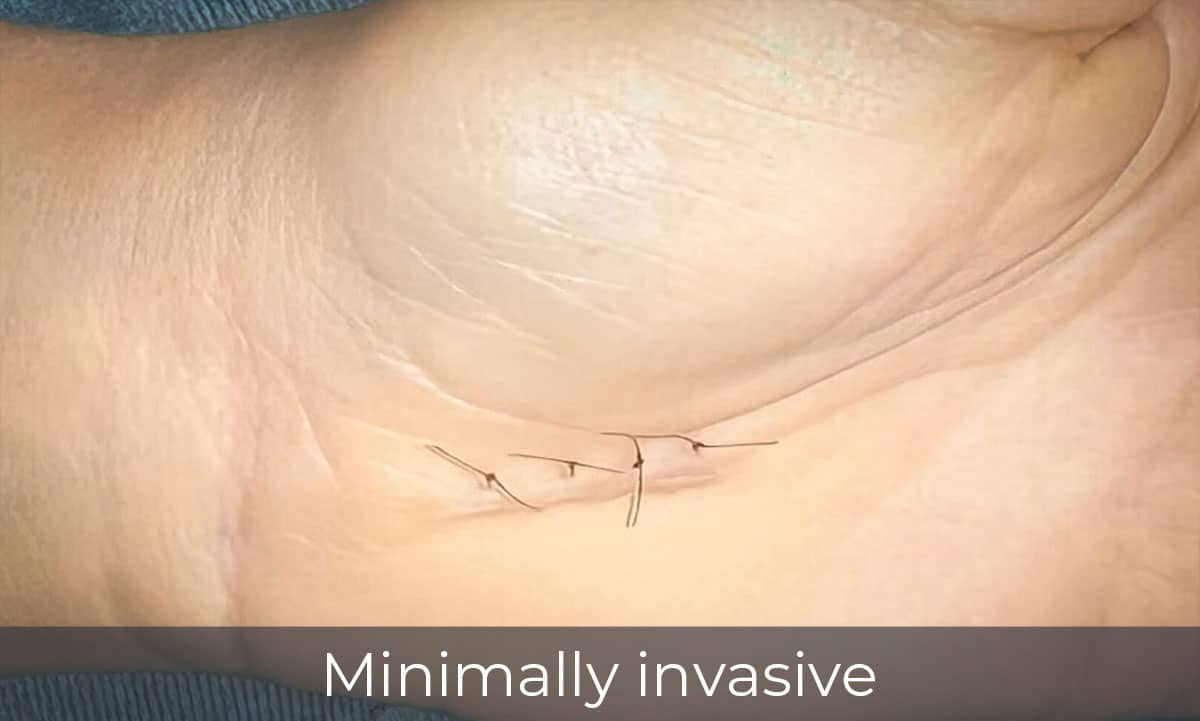
During an endoscopic surgical technique, a 5-7mm skin incision is made in the wrist’s flexor crease. The advantage of this is that the incision is outside the hand’s stress zone. Next, a small camera is inserted into the incision to view the carpal tunnel. This allows direct view of the flexor retinaculum, which can then be carefully severed.
The endoscopic surgical method is time-consuming and also requires specialised tools. This is why it’s rarely carried out in public hospitals or small practices. At our private clinic in Währung, we have specialised in this effective technique. The procedure can be carried out in the day clinic, without the need for full anaesthesia.
Endoscopic technique
How the procedure works:

STEP 1:
A 7mm skin incision is made in the wrist crease.

STEP 2:
The carpal tunnel is probed and cleaned.

STEP 3:
The endoscopic instrument (an integrated camera and scalpel) enter the incision.

STEP 4:
The flexor retinaculum (the roof of the carpal tunnel) becomes visible.
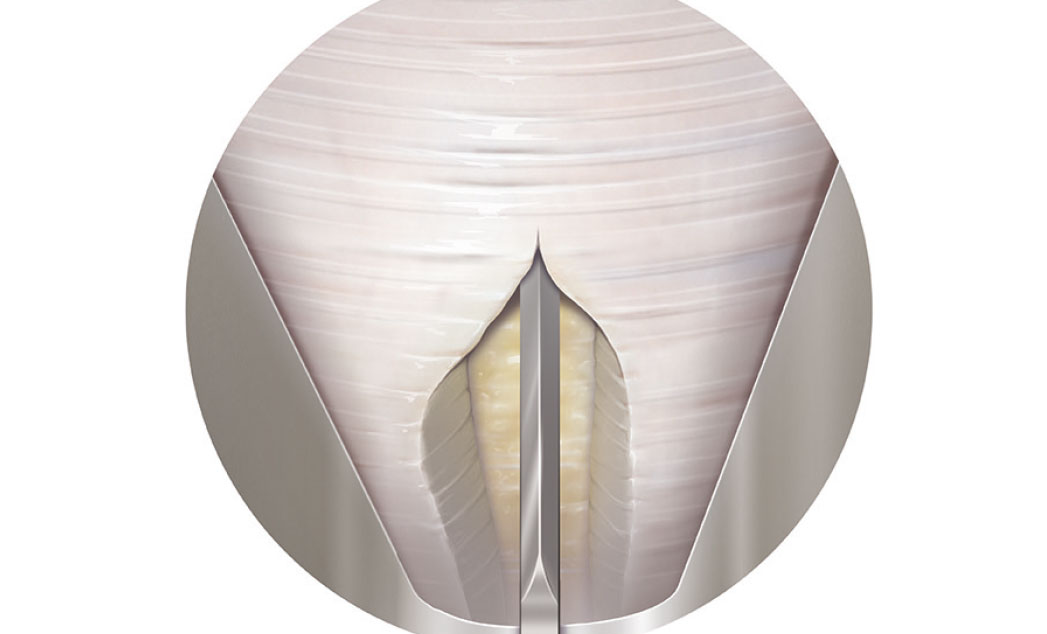
STEP 5:
Under direct observation, the flexor retinaculum is completely split using a hinged scalpel.

STEP 6:
A repeated check of the severed area is done under direct observation. The underlying fatty tissue is revealed.
Follow-up treatment
The wound is closed using a plastic surgical suture, then a bandage is applied. The wound is usually checked on the second day after the operation. By this time, the pain at night should be gone. The sutures are removed on the 12th day after the operation. A splint treatment is unnecessary, but you should avoid using the affected hand until the sutures have been removed.
Operating room images





Operating room images
Surgery video

CONTACT
Dr Georg C. Bézard, Senior Consultant
Arztpraxis Döbling
Döblinger Hauptstraße 16, 1190 Wien
Tulln Practice
Hauptplatz 29 / Eingang Donaugasse 2, Top 3, 3430 Tulln
Telephone: +43 (0) 660 3737 936
E-mail: office@drbezard.com
Internet: www.carpaltunnelsyndrom.at
Practice visits by appointment only


